Sinus Mechanisms
Please click a sub-section.
| Normal Sinus Rhythms | Sinus Bradycardia | Sinus Tachycardia | Sinus Arrhythmia | Sinoatrial Block | Summary | Show All | Hide All |
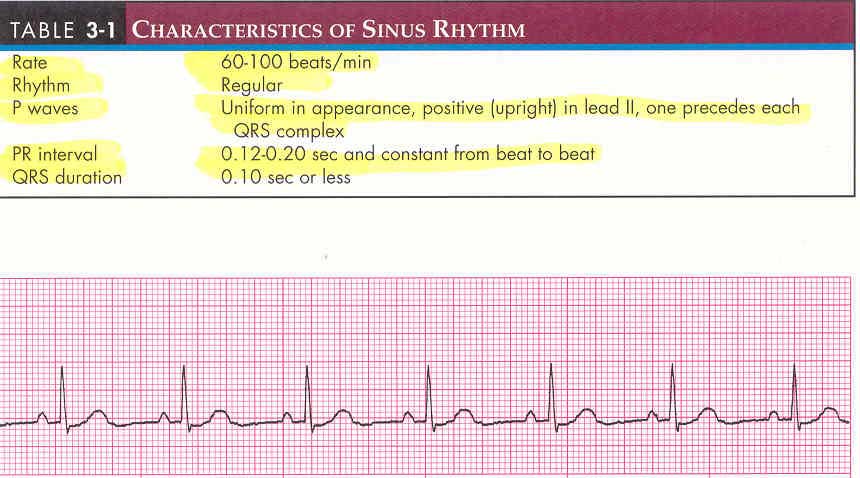
Normal Sinus Rhythms (NSR)
Sinus rhythm is the name given to the rhythm reflecting normal electrical activity - that is, the rhythm originates in the SA node and follows the normal pathway of conduction through the atria, AV junction, bundle branches, and ventricles resulting in atrial and ventricular depolarization.
Characteristics of NSR
Sinus Bradycardia (SB)
- The SA node discharges fewer than 60 bpm.
- Rhythm still originates in the SA node and follows the normal pathway of conduction.
Characteristics of SB

Causes and Clinical Significance
- SB may be normal in physically conditioned adults and during sleep.
- SB is the most common dysrhythmia associated with acute MI.
- Causes of SB may include: disease of the SA node, increased vagal tone such as vomiting, hypoxia, hypothermia, anorexia, hypothyroidism, hyperkalemia, glaucoma, sleep apnea, and meds, such as calcium channel blockers (verapamil, diltiazem), digitalis, and beta blockers (propranolol).
Interventions
- No intervention is necessary if patient is asymptomatic.
- If symptomatic due to SB, interventions may include Oxygen, IV access, and administration of Atropine and/or TCP (Transcutaneous Pacing).
Sinus Tachycardia (ST)
- The SA node discharges at a rate of greater than 100 bpm.
- Rhythm originates in the SA node and follows the normal pathway of conduction.
Characteristics of ST

Causes and Clinical Significance
- ST occurs as a normal response to the body's demand for increased oxygen due to fever, pain, anxiety, hypoxia, CHF, acute MI, infection, shock, hypovolemia, dehydration, exercise, and fright.
- ST may also occur as a result of administration of meds, such as epinephrine, atropine, dopamine, dobutamine, or subtances, such as nicotine, cocaine, and caffeine-containing beverages.
Interventions
- Interventions are directed at correcting the underlying cause. Examples include fluid replacement, relief of pain, removal of offending meds or substances, reducing fever and/or anxiety.
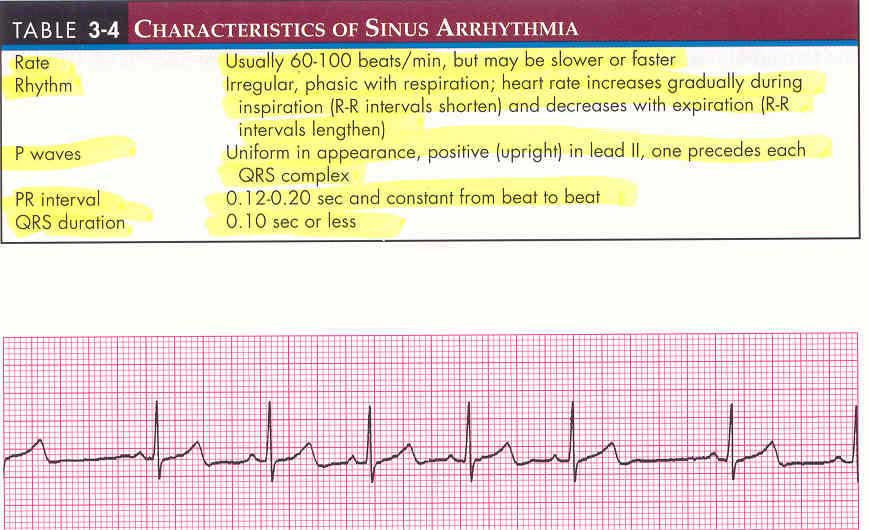
Sinus Arrhythmia
- Occurs when the SA node discharges irregularly.
- Originates in the SA node and follows the normal pathway of conduction.
Characteristics of Arrhythmia
Causes and clinical Significance
- If sinus arrhythmia is associated with a bradycardio rate, it is called sinus-brady arrhythmia. If associated with a tachycardic rate, it is called sinus tachy arrhythmia.
- Sinus arrhythmia is most commonly observed in infants and children, but may be seen in any age group.
- Non-respiratory sinus arrhythmia is more likely in older individuals and in those with heart disease. It is common after acute inferior wall MI. It may also be the result of effects of meds, such as digoxin and morphine.
Interventions
- Sinus arrhythmia does not require intervention unless it is accompanied by by a bradycardia that causes hemodynamic compromise. If hemodynamic compromise is present, IV atropine may be indicated.
Sinoatrial (SA) Block
- An impulse is initiated by the pacemaker cells within the SA node but is blocked as it exits the SA node.
- Thought to occur due to failure of the transitional cells in the SA node to conduct the impulse from the pacemaker cells to the surrounding atrium.
- Rhythmicity of the SA node is unaffected by the SA block, thus impulses are generated regularly.
- Because an impulse is blocked, the atria is not activated, which appears on the ECG as a single missed beat (P wave, QRS complex, T wave).
- The pause caused by the missed beat is the same as the distance between 2 P-P intervals of the underlying rhythm.
Characteristics of SA Block

Causes and Clinical Signifcance
- SA block is relatively uncommon but may occur as a result of: acute MI, digoxin, quinidine, procainamide, CAD, CHF, myocarditis, increased vagal tone.
- If episodes are frequent and/or accompanied by a slow heart rate, patient may show s/s of hemodynamic compromise (HTN, CP, SOB, change in mental status), left ventricular failure, decrease in urinary output, cold and clammy skin.
Interventions
- If no clinical s/s exist, the patient is observed.
- If s/s of hemodynamic compromise are present and are the result of med toxicity, the offending agents should be withheld.
- If SA block is frequent, IV atropine, temporary pacing, or insertion of PPM may be warranted.
Sinus Mechanisms: Summary of Characteristics

↑ Top of Page ↑